Patient Information

Frozen shoulder
Print this page
![]()
Information in this booklet is intended to be used as a guide. It gives you an idea about how frozen shoulder can be managed.
You should remember that every case is different, and symptoms and management can vary from person to person.
Frozen shoulder is a very painful condition that means your shoulder is stiff and painful. It can make everyday tasks like getting dressed, reaching up to brush your hair or tucking your shirt in very difficult.
Frozen shoulder is also known as ‘adhesive capsulitis’. There are two types of frozen shoulder, primary and secondary. Primary frozen shoulder generally has three phases, pain, stiffness and recovery.
There is often no trigger for a frozen shoulder and a full recovery can take up to two years. Management includes pain relief, exercise and advice from a physiotherapist.
What is frozen shoulder?
Frozen shoulder is a very painful condition that means your shoulder is stiff and painful. Everyday tasks like getting dressed, reaching up to brush your hair or tucking your shirt in are very difficult.
Frozen shoulder happens when the tissue around your shoulder joint becomes inflamed.
This tissue then gets tighter and shrinks, which causes pain and limited movement.
Primary frozen shoulder is not related to bony problems such as arthritis or muscle problems.
It is more common in people with diabetes, but you do not have to have diabetes to get a frozen shoulder.
There are two types of frozen shoulder:
Primary - no apparent cause or trigger.
Secondary - onset following an injury or surgery of the shoulder (secondary to another cause).
Frozen shoulder is also known as ‘adhesive capsulitis’.
Complete recovery from frozen shoulder can take several years, but it is managed with pain relief, exercise and advice from a physiotherapist. They will advise you about how to keep moving, control your symptoms and continue with your normal life. Sometimes injections or surgery are offered if symptoms are not settling.
Why me?
It’s not always clear why someone gets frozen shoulder. It is thought to affect people who are 40 to 60 years old and is more common in women.
Some people develop frozen shoulder after a shoulder or arm injury, such as a broken bone, or after shoulder surgery. This might be because your shoulder and arm has been kept still after an injury or surgery, which may cause your shoulder capsule to stiffen up.
If you have diabetes you are more likely to develop frozen shoulder in one or both of your shoulders. It is not known why people with diabetes are more likely to develop this.
Other health conditions such as heart disease, lung disease, an overactive thyroid gland, Parkinson’s disease, a stroke or a condition called Dupytren’s contracture, may also increase the risk of developing frozen shoulder. Sometimes there is no obvious reason for this to develop.
Symptoms
A frozen shoulder normally gives you both pain and stiffness. The symptoms move through three stages:
Pain: Your shoulder feels stiff and achy, then becomes more painful. Pain is often worse at night and lying on the affected shoulder is very difficult. This stage can last between two and nine months
Stiffness: The stiffness becomes the main problem; the pain does not usually become any worse and may start to settle down. This stage can last between four and 12 months.
Recovery: In the final recovery stage, you gradually notice better movement in your shoulder and the pain fades, although you may notice the occasional increase in pain at times. This stage can last from five months to four years. You may not get full movement of your shoulder, but you will still be able to do many more tasks.
It is important to remember that everybody is different and other health issues, such as diabetes, can cause each stage to last longer.
Diagnosis and investigations
A frozen shoulder is diagnosed from the signs and symptoms that you describe and an assessment of the shoulder, neck and elbow by a healthcare professional.
Sometimes an x-ray is indicated; you cannot see a frozen shoulder on an x-ray, but it can rule out other issues, such as arthritis.
Early treatment can help to prevent long-term stiffness of your shoulder joint.
Blood tests are not used to diagnose frozen shoulder, but they may be needed to rule out other conditions, such as:
Diabetes
Polymyalgia rheumatica
Infection.
Will it get better?
Recovery from frozen should varies between people. You may find that pain settles down, but you still notice stiffness when you move your shoulder fully, such as reaching right up or behind you.
Your healthcare professional will work with you to ensure any discomfort is managed as much as possible.
We work with a team of advanced clinical practitioners and orthopaedic consultants who can review your case if symptoms do not improve within the expected period of your time.
A frozen shoulder can take at least one and a half to two years to get better; sometimes it can be up to five years. However, the pain and stiffness will usually go away eventually.
Surgery for frozen shoulder is rare.
Management
Treatment for a frozen shoulder varies depending on the stage of the condition and the severity of your pain and stiffness. The aim of treatment is to keep your joint as mobile and pain-free as possible while your frozen shoulder resolves.
While treatment will not necessarily speed up your recovery, it can make it more bearable.
You should only move as much as you feel is manageable. The level of pain you experience during or after movements can be a helpful guide. You should not stop moving altogether.
Treatment during this stage is mainly focused on relieving the pain.
Early stage (pain): The early stage of a frozen shoulder is the most painful stage.
Later stages (stiffness): After the painful stage, stiffness is the main symptom of a frozen shoulder.
Medication for pain control
Controlling your pain allows you to continue to function and carry out your daily activities more comfortably.
Your GP may have already discussed medication to help with your pain and the correct ways to take pain relief. They may recommend that you take it as a short course rather than ‘as and when’ the pain is bad. This often includes paracetamol, co-codamol (Zapain), and non-steroidal anti-inflammatory medication such as ibuprofen. Please always read the instructions before using these products.
We work with a team of orthopaedic advanced practitioners and consultants. If you do not respond to physiotherapy, we can escalate your care, such as considering steroid injections.
Steroid injections
Steroid injections are sometimes used to facilitate physiotherapy exercises. They offer a window of opportunity to reduce symptoms, to allow participation in the exercises. Injections are only offered alongside physiotherapy.
Steroid injections can be discussed with your healthcare professional.
Corticosteroid injections can help to relieve pain and improve the movement in your shoulder. However, the effect of injections can only be short-lasting if used in isolation. Corticosteroid injections will also not be used once the pain has faded from your shoulder and only the stiffness remains.
Too many corticosteroid injections are not recommended, therefore you can only have this type of treatment up to three times in one year. You will need at least four to eight weeks between injections.
Physiotherapy
Referral to a physiotherapist will help you to keep the movement in your shoulder.
Physiotherapy treatments can include stretching exercises, strengthening exercises, advice about posture and pain relief.
You may find that physiotherapy alongside other treatments, such as pain relief or an injection, lets you do your exercises more comfortably.
If you have a frozen shoulder, it is important to keep your shoulder joint moving with regular, gentle exercise. Not using your shoulder can cause your muscles to weaken and may make the stiffness worse. Therefore, you should continue to use your shoulder as normal where possible. Examples of exercises can be found at the end of the booklet.
Surgery
Surgery for frozen shoulder is not usually necessary, but you may be referred for surgery if other treatments have not worked after six months.
You could be referred to an orthopaedic consultant (surgeon), a specialist in conditions that affect the muscles and bones.
There are two possible surgical procedures:
Manipulation under anaesthetic (MUA)
You can have your shoulder manipulated (moved) while you are under general anaesthetic. During this procedure, your shoulder is moved and stretched while you are asleep to regain the movement.
Afterwards, you will usually require physiotherapy to help maintain mobility in your shoulder. Manipulation may be used if you are finding the pain and disability from your shoulder difficult to cope with.
Arthroscopic capsular release
An alternative procedure to manipulation, is an arthroscopic capsular release; this is a type of keyhole surgery.
During an arthroscopic capsular release surgery, your surgeon will use a special probe to ‘release’ your contracted shoulder capsule and remove any scar tissue that has formed in your shoulder capsule.
As with manipulation, you will need to have physiotherapy after having arthroscopic capsular release surgery, to help you to regain a full range of movement in your shoulder joint.
Exercises
Here are some exercises that you may wish to try. Please bear in mind that it is normal to feel some stretch and even a bit of discomfort when doing exercises, but it is important to keep a balance. If pain is increasing beyond what feels tolerable for you, or if you are experiencing new symptoms, you should stop. Do not carry on just to finish the set.
If you experience pain that lasts for more than 30 minutes, try reducing the number of repetitions in each set or doing them with less force.
If you feel any severe pain during or after doing any of these exercises, you should stop doing them.
You may find it helpful to do your exercises after using a heat pack and within 30 to 60 minutes of taking your regular pain relief.
Start by doing them one to two times per day.

- Standing next to a table or other flat surface, bend over while leaning on the flat surface with your symptom-free forearm.
- Let your sore arm hang straight down, relaxed
Swing your arms; forward and backwards, side to side and around in small circles. - Repeat the above ten times.
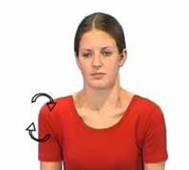
- Seated or standing, let your arms hang by your sides, relaxed.
- Roll your shoulders forward and then backward.
- Repeat the above ten times in both directions.

- Using a shoulder pulley, sit facing a wall with each hand holding onto either end of the rope.
- Lift your sore arm as far as symptoms allow by pulling down the rope with the other hands.
- Release and return to the starting position.
- Repeat the above for 30 seconds to two minutes.
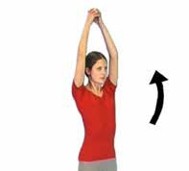
- Seated or standing, relax your arms down with your hands clasped in front of you.
- Lift your hands towards the ceiling as far as symptoms allow - your sore arm is helped by your other arm.
- Don’t worry if you don’t move as far as the picture shows - just move to where your symptoms allow.
- Repeat the above ten times.

- Lie on your back with your elbows against your body and at a right angle.
- Holding a light stick in your hands, move the stick sideways pushing the sore arm outwards.
- Keep your elbows tucked into your sides and your shoulders relaxed so they are not raising to your ears.
- Repeat the above ten times.

- From standing, grip one end of a stick with your sore arm.
- Lift your sore arm out to the side using the stick to help it move.
- You may not move as far as the picture shows
- just move to where your symptoms allow. - Try to keep your shoulders relaxed and your shoulder blade down/back. Don’t let your shoulder blades rise towards your ears.
- Repeat the above ten times.

- Standing, bring your sore arm behind your back as far as you are able, stretching towards the opposite buttock.
- Repeat the above ten times.

- Seated or standing, stretch your sore arm over to the opposite shoulder by pushing it at the elbow with your other arm.
- Hold the stretch for approximately 20 seconds and then relax.
- Repeat the above ten times.

- Lie on your back with your elbows bent.
- Hold the wrist of your sore arm with your other hand.
- Lift your sore arm towards the wall behind you as far as symptoms allow, assisting with your other hand.
- Return to the start position slowly.
- Repeat the above ten times.
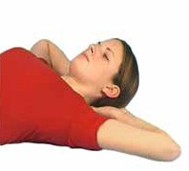
- Lie on your back with both hands behind your neck with elbows pointing towards the ceiling.
- Move the elbows apart as far as symptoms allow down towards the floor.
- Hold for three to five seconds if comfortable.
- Return to the starting position.
- Repeat the above ten times.

Gently turn your head to each side - repeat ten times.

Gently tilt your head to each side - repeat ten times.

Look down then return to the upright position - repeat 10 times.
Keep your shoulders relaxed and don’t hold your breath as you move.
Your Health Notts
It is always important to consider other factors that can contribute to musculoskeletal problems and may limit your recovery. The most common factors that can affect your health and wellbeing include smoking, alcohol, weight, stress and general fitness.
There is an excellent resource now available to Nottinghamshire County residents that offers information and guidance on:
- Stopping smoking
- Losing weight
- Alcohol reduction
- Increasing physical activity.
Please visit the Your Health Notts website to find out more or self-refer to this service.
Further sources of information
This document is intended for information purposes only and should not replace advice that your relevant health professional would give you.
External websites may be referred to in specific cases. Any external websites are provided for your information and convenience. We cannot accept responsibility for the information found on them.
Patient Experience Team
The Patient Experience Team (PET) is available to help with any of your compliments, concerns or complaints, and will ensure a prompt and efficient service.
Contact Patient Experience.
Approved
October 2025
Review date
October 2027
Document Id
PIL202510-01-FSHO
Service / Department
Musculoskeletal (MSK)
Other formats
Patients who would like this information in an alternative format, or need help communicating with us, please contact our patient experience team.


