Patient Information

Meniscal tears
Print this page
![]()
Information in this booklet is intended to be used as a guide. It gives you an idea about the management of meniscal tears.
You should remember that every case is different, and symptoms and management can vary from person to person.
The menisci are ‘c’ shaped cartilage structures in the knee. They act like thick pads which sit between the thigh bone (femur) and shin bone (tibia). Each knee joint has an inner and outer meniscus. They have several functions including shock absorption, increasing joint stability and spreading load through the joint.
The main symptoms of a meniscal tear are pain, swelling, locking and/or reduced movement. However, many people with meniscal tears do not have any symptoms at all. It is important to remember that even if you have a meniscal tear, this does not always mean that the tear is causing your pain; your symptoms may be caused by something else. The tear may have been there before your current symptoms started.
Treatment will depend on the type and size of tear, the symptoms it causes and the general condition of the knee. Many people with meniscal tears benefit from physiotherapy to improve the strength and condition of the knee.
Surgery may be required if you have a large tear with severe symptoms, including locking and giving way. However, surgery is not always successful, especially for degenerative tears or in patients who have arthritis in the knee joint already.
Patients with meniscal tears who are treated without surgery tend to do just as well as patients who have surgery.
What is a meniscal tear?
In the knee, there are two types of cartilage; one of the types is called meniscus. There are two menisci that are like thick pads which sit in-between the bones. They act like shock absorbers and help to protect the bones in the knee joint from the impacts caused by everyday activities.
There are two types of meniscal tears - acute (due to a specific injury, normally involving a large force), and degenerative (not due to a specific injury).
A meniscus can be torn if a large force is placed on the knee, for example when you twist your knee while standing on that leg. It is a common injury among footballers.
These degenerative tears are common in people who are aged over 40. In fact, it is well known that half of people over the age of 50 will have a degenerative tear, yet most show no symptoms at all.
Symptoms
The main symptoms of a meniscal tear are pain, swelling and reduced movement. You may not be able to fully straighten the knee. The symptoms can be worse with activity, and you may experience short, sharp pains in the knee if you twist it.
If the tear is larger, or part of the meniscus becomes loose, the knee may ‘lock’ in a bent position. You may need to move your leg with your hands to straighten it. You may also feel like the knee gives way.
It is important to remember that even if you have a meniscal tear, this does not always mean that the tear is causing your pain or that the tear needs repairing.
In one recent study, MRI scans found some sort of problem in the knees of nine out of 10 people over the age of 50. However, only three in 10 people had knee pain. Of those people who did have meniscal tears on a scan, most had no pain.
Diagnosis and investigations
Meniscal tears can often be diagnosed by a healthcare professional based on the information you give about your symptoms, combined with some simple tests.
Your healthcare professional may request an x-ray. This will not show the meniscus itself but will help to check if there are any issues with the bones, such as osteoarthritis. A diagnosis can be confirmed by an MRI scan, but these are only usually required if you are experiencing severe pain or symptoms such as locking and giving way, or it is felt that you may need to see a surgeon.
Will it get better?
The cartilage in the meniscus does not have a very good blood supply. This means that it does not heal very well, particularly if the meniscus is generally worn.
Small meniscal tears on the outer edge of the meniscus may heal over time, as there is a better blood supply in this area. They may take two to three months to heal fully. Larger tears, or tears closer to the centre of the meniscus, do not tend to heal. However, once the initial pain and swelling subside most Meniscal Tears cause only mild symptoms.
We work with a team of advanced clinical practitioners and orthopaedic consultants who can review your case if symptoms do not improve within an expected period of time.
Steroid injections are sometimes used to facilitate physiotherapy exercises. They offer a window of opportunity of reduction in symptoms to allow participation of the exercises. Injections are only offered in conjunction with physiotherapy.
Management
Treatment will depend on the size and type of tear, the symptoms it causes and the general condition of the knee.
When your knee first starts hurting, you can use the PRICE approach for one to two weeks:
Protect from further injury.
Rest the knee for one to two days (use crutches if required).
Ice (for 10 minutes at a time, regularly throughout the day).
Compression (with a stretch bandage).
Elevate.
After this, it is important to get active again as quickly as possible to avoid the knee becoming weak and stiff.
Physiotherapy
Many people with meniscal tears benefit from exercises to improve the strength and condition of the knee. This helps to reduce the strain and improve the overall function of the knee.
Several studies have shown that, in the longer term, most patients with meniscal tears who were treated without surgery do just as well as patients who had surgery.
Medication for pain control
Controlling your pain allows you to continue to function and carry out your daily activities more comfortably.
Your GP may have already discussed medication to help with your pain and the correct ways to take pain relief. They may recommend that you take it as a short course rather than ‘as and when’ the pain is bad. This often includes paracetamol, co-codamol (Zapain), and non-steroidal anti-inflammatory medication such as ibuprofen. Please always read the instructions before using these products.
We work with a team of orthopaedic advanced practitioners and consultants. If you do not respond to physiotherapy, we can escalate your care, such as considering steroid injections.
Steroid injections
If the pain is not manageable, a steroid injection may be offered. This can provide short-term pain relief, which can allow participation in physiotherapy exercises. Steroid injections are not a long-term solution and will only be offered in conjunction with your physiotherapy treatment. This can be discussed with your healthcare professional.
Surgery
Surgery may be required if you have a large tear with severe symptoms, including locking and giving way.
Surgery may involve:
Repairing the torn meniscus.
Removing parts, or all, of the damaged meniscus (meniscectomy) and any fragments of loose meniscus from the knee joint.
However, surgery is not always successful, especially for degenerative meniscal tears in patients with osteoarthritis in the knee. It is also thought that removing parts, or all, of the meniscus can cause the remaining cartilage in the knee to wear more quickly.
Exercises
The following exercises may help you recover from your meniscal tear.
When your symptoms are new or more severe:
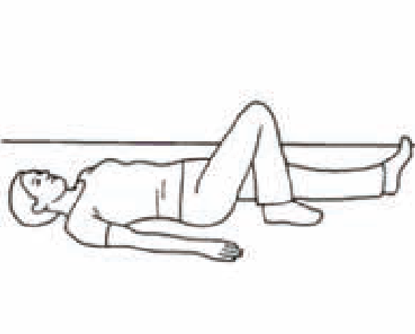
Lying on your back, bend your affected leg.
Hook the foot of your good leg around the ankle of your affected leg to increase the bend.
Hold for five seconds, then straighten your leg.
Repeat the above 10 times for a total of two to three sets.

Lie on your back with your good leg bent and your affected leg straight.
Exercise your straight leg by pulling the toes up, straightening the knee and lifting the leg 20cm off the bed or floor.
Hold for five seconds, then slowly lower your leg back down to the bed.
Repeat the above 10 times for a total of two to three sets.
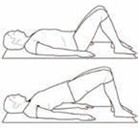
Lie on your back with both knees bent.
Squeeze your buttocks together and lift your bottom off the floor, keeping your back straight.
Hold for a few seconds, then return to the starting position.
Repeat the above 10 times for a total of two to three sets.
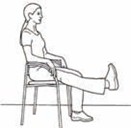
Sit up straight in a chair.
Fully straighten your affected knee and hold for a few seconds.
Slowly lower your foot back to the starting position.
Repeat the above 10 times for a total of two to three sets.
This exercise can be made harder by adding a small weight to your ankle.

Lie face down with your hips straight and your knees together.
Bend your affected knee as far as possible and hold for a few seconds.
Slowly lower your foot back to the starting position.
Repeat the above 10 times for a total of two to three sets.
This exercise can be made harder by adding a small weight to your ankle.
When your acute symptoms have settled, and you want to further strengthen your knee:

Lean against a wall with your feet about 20cm from the wall.
Keeping your back against the wall, slowly slide down the wall until your hips and knees are at right angles.
Hold for a few seconds, then slowly return to your starting position.
Repeat the above 10 times for a total of two sets.
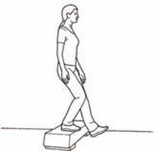
Standing on a step, slowly lower yourself to the next step by bending your affected knee.
Try to keep your knee lined up over your second toe as you bend.
Return to the starting position.
Repeat the above 10 times for a total of two to three sets.
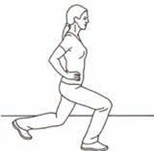
Standing straight, take a step forward with your affected knee and bend your knees (as if to lunge).
Try to keep your front knee lined up over your second toe as you step forward.
Return to the starting position.
Repeat the above 10 times for a total of two to three sets.

Lie on your back with both knees bent.
Squeeze your buttocks together and lift your bottom off the floor, keeping your back straight.
Keeping your pelvis level, shift your weight onto one leg.
Straighten the other leg, then slowly lower it back down.
Repeat the above 10 times on each leg.
Your Health Notts
It is always important to consider other factors that can contribute to musculoskeletal problems and may limit your recovery. The most common factors that can affect your health and wellbeing include smoking, alcohol, weight, stress and general fitness.
There is an excellent resource now available to Nottinghamshire County residents that offers information and guidance on:
- Stopping smoking
- Losing weight
- Alcohol reduction
- Increasing physical activity.
Please visit the Your Health Notts website to find out more or self-refer to this service.
Further sources of information
This document is intended for information purposes only and should not replace advice that your relevant health professional would give you.
External websites may be referred to in specific cases. Any external websites are provided for your information and convenience. We cannot accept responsibility for the information found on them.
Patient Experience Team
The Patient Experience Team (PET) is available to help with any of your compliments, concerns or complaints, and will ensure a prompt and efficient service.
Contact Patient Experience.
Approved
October 2025
Review date
October 2027
Document Id
PIL202510-01-MET
Service / Department
Musculoskeletal (MSK)
Other formats
Patients who would like this information in an alternative format, or need help communicating with us, please contact our patient experience team.


