Patient Information

Rotator cuff related shoulder pain (RCRSP)
Print this page
![]()
Information in this booklet is intended to be used as a guide. It gives you an idea about how rotator cuff related shoulder pain (RCRSP) can be managed.
You should remember that every case is different, and symptoms and management can vary from person to person.
Previously known as impingement syndrome, rotator cuff tendinopathy or subacromial pain syndrome.
The shoulder joint is the most mobile joint in your body. It is a ball and socket joint that allows for lots of movement involved and needed for washing, dressing and reaching. However, to allow for this movement the shoulder has less ‘bony support’ than other joints like the hip and requires muscles and tendons to provide stability and control.
A group of four muscles and their tendons make up the rotator cuff, which controls movement and helps to hold the joint together.
Shoulder pain is very common and affects between 15-25% of adults; this percentage increases as we get older. Shoulder pain can be annoying and painful, but it is rarely due to a serious condition.
RCRSP refers to a variety of shoulder pathologies related to the rotator cuff. It is rarely a singular pathology causing symptoms, and this term describes them.
The condition can normally be diagnosed by your reported symptoms and an assessment completed by your healthcare professional. Further investigations are often not needed. If the diagnosis is unclear, then an x-ray or ultrasound can be performed to aid the diagnosis.
Approximately 80% of patients are treated successfully with conservative (non- surgical) treatment. Physiotherapy can be very helpful in improving your symptoms and is normally the only treatment required. The use of exercises and education can help to reduce your pain and increase your movement by strengthening the rotator cuff and improving the stability of the shoulder.
What is rotator cuff related shoulder pain (RCRSP)?
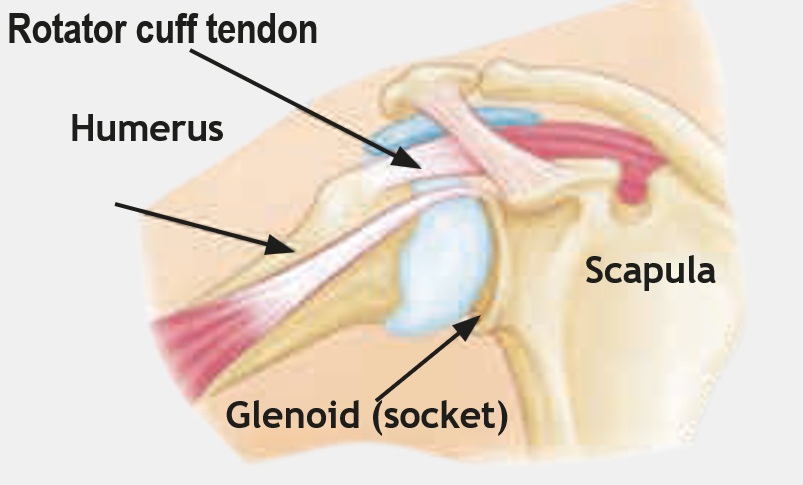
The rotator cuff provides stability to the ball and socket joint. The picture below shows the rotator cuff travelling through the tunnel between the acromion (the roof of the shoulder blade) and the ‘ball’ of the humerus (the bone in the top of your arm).
If the control or strength of these muscles is affected or reduced, then they can become stressed. This can cause these muscles to become painful.
Rotator cuff related shoulder pain as a condition does not cause any serious damage to the muscles and responds well to conservative treatment, such as simple home exercises.
Why me?
Anyone can develop RCRSP, and many factors can contribute towards its development. These can include:
Muscle weakness or imbalance.
Injury.
Shoulder stiffness.
Posture.
Age-related change of the muscles/tendons, or joints of the shoulder.
Decreased activity.
Stress, anxiety and poor sleep.
Symptoms can develop gradually or follow from an injury. They are more commonly experienced in individuals older than 45 years of age. Often there is no clear cause of the pain.
Overuse or underuse of the shoulder can be a cause of pain. People who complete regular overhead activity, such as painting and decorating, or work with an outstretched arm, such as hedge trimming, can contribute to developing symptoms. This is often due to the mechanical element.
Symptoms
As RCRSP includes a few different conditions, the symptoms can vary. They can range from very mild to more intense symptoms and can include:
An ache or pain in the shoulder or upper arm.
Pain on movement of the shoulder, especially above head height.
Reduction in movement, such as reaching behind your back, putting your arm in a coat or reaching for a seatbelt.
Weakness or stiffness when lifting heavy items.
Discomfort when lying on the painful side.
Diagnosis and investigations
Rotator cuff related shoulder pain can be diagnosed from the signs and symptoms that you describe. Assessment of the shoulder, neck and arm by a healthcare professional will help to inform this diagnosis.
Depending on your presentation, an x-ray and/or ultrasound may be indicated to provide additional information to aid the diagnosis and recommend treatment. Investigations only provide information to support the clinical examination.
Ultrasound scans
An ultrasound scan looks at the 'soft tissues' around the shoulder, such as the muscles, tendons and bursa. It is important to remember that tears can be found on ultrasound scans, but this does not mean the tear(s) are responsible for the symptoms you are experiencing.
X-rays
An x-ray looks at the bones of the shoulder, assessing the quality of the joint and the surface of the bones.
Will it get better?
Approximately 80% of patients with this condition are treated successfully with conservative (non-surgical) management. This will include exercises, some of which are demonstrated towards the end of this booklet.
We work with a team of advanced clinical practitioners and orthopaedic consultants who can review your case if symptoms do not improve within an expected period of time.
Steroid injections are sometimes used to facilitate physiotherapy exercises. They offer a window of opportunity for a reduction in symptoms to allow participation in the exercises. Injections are only offered in conjunction with physiotherapy.
Management
RCRSP is treated with a variety of different management techniques. Below is a list of ways you can help yourself:
Rest. Relative rest from the activity or movement that hurts. This does not mean stopping all shoulder movements, but perhaps reducing how often you do the painful activities.
Pacing activity. Taking regular breaks from difficult or repetitive activities, such as lifting, if possible.
Pain relief. As required and as recommended by your GP or pharmacist. This is often a combination of analgesia and anti-inflammatories.
Movement. Continue to keep your shoulder moving. Even if it is just changing position, try to do so every 30 minutes or so.
Active. Being active for 30 minutes in your day can make a big difference in your overall health and reduce your pain. Sedentary and inactive lifestyles increase the risk of developing pain and can also delay your recovery
Work. If you use a computer, make sure that you do not have to stretch your arm forward to use your mouse, and arrange your workstation so that everything that you use frequently is within easy reach
Posture. Try not to ‘slouch’ in your chair. Sit with your arm supported on a pillow or the armrest.
Exercise. See the exercise section for suggestions.
Medication for pain control
Controlling your pain allows you to continue to function and carry out your daily activities more comfortably.
Your GP may have already discussed medication to help with your pain and the correct ways to take pain relief. They may recommend that you take it as a short course rather than ‘as and when’ the pain is bad. This often includes paracetamol, co-codamol (Zapain), and non-steroidal anti-inflammatory medication such as ibuprofen. Please always read the instructions before using these products.
Steroid injections
Steroid injections are sometimes used to facilitate physiotherapy exercises.
The steroid injection for RCRSP is into the subacromial bursa so it is considered a soft-tissue injection. It is therefore not recommended to have more than two of these.
They offer a window of opportunity to reduce symptoms, to allow participation in the exercises. Injections are only offered alongside physiotherapy. Steroid injections can be discussed with your health care professional.
Surgery
Surgery is rarely needed. The operation aims to increase the space under the acromion. This is an arthroscopic (keyhole) surgery and is called a subacromial decompression (SAD).
Exercises
All the exercises advised can be tried at home once a day. If they are easy, then you can increase how many times you do them to two to three times per day. If they are painful or cause new symptoms, then please reduce how many you do or stop them if necessary.

Standing next to a wall with your elbow bent and tucked into your side.
Push the back of your hand and wrist against the wall, making sure your elbow stays tucked in.
Squeeze your shoulder blades together.
Push enough to feel the muscle around your shoulder and shoulder blade switch on.
Push for five seconds and then relax.
Repeat five to ten times.

Stand or sit next to a wall with your affected arm next to the wall.
Let your arm relax by your side.
Push your arm outwards against the wall.
Push for five seconds and then relax.
Repeat five to ten times.

You can do this exercise standing up, or if this is too difficult, then you can lie down on your back and do it.
Holding a small towel in both hands, keep it tight.
Lift the towel out in front and then above you as far as you can.
If you cannot get as far as the picture, then just lift as far as you can comfortably.
Slowly lower back down and relax your shoulder.
Repeat five to 10 times (increase the number if it is easy to complete).
Your Health Notts
It is always important to consider other factors that can contribute to musculoskeletal problems and may limit your recovery. The most common factors that can affect your health and wellbeing include smoking, alcohol, weight, stress and general fitness.
There is an excellent resource now available to Nottinghamshire County residents that offers information and guidance on:
- Stopping smoking
- Losing weight
- Alcohol reduction
- Increasing physical activity.
Please visit the Your Health Notts website to find out more or self-refer to this service.
Further sources of information
This document is intended for information purposes only and should not replace advice that your relevant health professional would give you.
External websites may be referred to in specific cases. Any external websites are provided for your information and convenience. We cannot accept responsibility for the information found on them.
Patient Experience Team
The Patient Experience Team (PET) is available to help with any of your compliments, concerns or complaints, and will ensure a prompt and efficient service.
Contact Patient Experience.
Approved
October 2025
Review date
October 2027
Document Id
PIL202510-01-SPS
Service / Department
Musculoskeletal (MSK)
Other formats
Patients who would like this information in an alternative format, or need help communicating with us, please contact our patient experience team.


