Patient Information

Rotator cuff tears
Print this page
![]()
Information in this booklet is intended to be used as a guide. It gives you an idea about how rotator cuff tears can be managed.
You should remember that every case is different, and symptoms and management can vary from person to person.
The rotator cuff is a group of tendons that connect four muscles from around your shoulder blade (scapula) to the bone at the top of your arm (humerus). These muscles help to keep the ball in the socket as you lift your arm.
Functionally the rotator cuff lifts and rotates the arm.
The rotator cuff is made of strong bands called tendons that help your shoulder to move. Over time, these tendons can become less strong and may get small or big tears. Sometimes this can happen slowly as you get older and sometimes it can happen quickly, like after a fall. Pain can come all of a sudden or develop over time.
The main symptoms of a rotator cuff tear are pain, weakness and reduced movement. However, many people with rotator cuff tears do not have any symptoms at all. It is important to remember that even if you have a rotator cuff tear, this does not always mean that the tear is causing all your pain. Your symptoms may be caused by something else.
Treatment will depend on the size and type of tear, the symptoms and the general condition of your shoulder. Many people with rotator cuff tears benefit from physiotherapy to improve the strength and condition of their shoulder. Surgery may be offered.
What is a rotator cuff tear?
Your shoulder is a ball-and-socket joint. The ball sits at the top of the bone of your upper arm. The socket sits on the edge of your shoulder blade.
The rotator cuff is a group of tendons that connect four muscles around your shoulder blade to the top of your arm. The rotator cuff works with the other big muscles around your shoulder and can improve the movement of the shoulder when you use your arm.
There are two types of rotator cuff tears. One due to trauma, like a fall, is known as an acute tear. And another due to age, called a degenerative tear.
The chances of having a rotator cuff tear increase with age. These tears are common in people over 65. Up to 50% of people over 65 have a rotator cuff tear, many of whom do not have symptoms.
Diagnosis and investigations
Rotator cuff tears can be diagnosed from the signs and symptoms that you describe. Assessment of the shoulder, neck and arm by a healthcare professional will help to inform this diagnosis.
Depending on your presentation, imaging may be indicated to provide additional information to aid the diagnosis and recommend treatment. Investigations only provide information to support the clinical examination.
Ultrasound scans
An ultrasound scan looks at the 'soft tissues' around the shoulder, such as the muscles, tendons and bursa. It is important to remember that tears can be found on ultrasound scans, but this does not mean the tear(s) are responsible for the symptoms you are experiencing.
X-rays
An x-ray looks at the bones of the shoulder, assessing the quality of the joint and the surface of the bones.
Additional Investigations
An MRI scan may be indicated if your presentation is complex, however this is rare. There are no blood tests for rotator cuff tears.
Symptoms
The main symptoms of a rotator cuff tear are pain, weakness and reduced movement in the shoulder. Sometimes the pain can spread to the shoulder blade or down into the upper arm.
If the rotator cuff is torn, the ball may not move as smoothly in the socket. This can cause irritation of the soft tissues around the shoulder joint. This usually causes a short, sharp pain when the arm is put in certain positions, most often when it is above your head or behind your back.
It is important to remember that even if you have a rotator cuff tear, this does not always mean that the tear is causing all your pain. Your symptoms may be caused by something else.
Will it get better?
It is unlikely that any tears in the rotator cuff will heal, particularly if degenerative in nature. However, symptoms often improve without surgery.
Symptoms can settle with conservative (non-surgical) treatment, which can improve the function of your shoulder. This will include exercises, some of which are demonstrated towards the end of this booklet.
It may take between three and six months of consistent exercise to get better, but this is normal.
We work with a team of advanced clinical practitioners and orthopaedic consultants who can review your case if symptoms do not improve within an expected period.
Steroid injections are sometimes used to facilitate physiotherapy exercises. They offer a window of opportunity for a reduction in symptoms to allow participation in the exercises. Injections are only offered in conjunction with physiotherapy.
Surgery is only offered with acute tears within six weeks of the injury or with chronic problems if conservative management has failed. The operation aims to increase the space under the acromion. If the quality of the tendon is poor (degenerative), then a repair is often not an option, as the surgery is likely to fail.
Management
Rotator cuff tears are treated with a variety of management techniques. Treatment will depend on the size and type of tear, the symptoms it causes and the general condition of the shoulder.
Physiotherapy
Many people with rotator cuff tears benefit from exercises to reduce stiffness and improve the strength of the shoulder. This will not help the tendon heal, but it will help the weakness and reduced function caused by the tear. It will also help reduce the chances of you suffering from any inflammation of the tendons or developing a stiff shoulder.
Medication for pain control
Controlling your pain allows you to continue to function and carry out your daily activities more comfortably.
Your GP may have already discussed medication to help with your pain and the correct ways to take pain relief. They may recommend that you take it as a short course rather than ‘as and when’ the pain is bad. This often includes paracetamol, co-codamol (Zapain), and non-steroidal anti-inflammatory medication such as ibuprofen. Please always read the instructions before using these products.
Holistic management
There are multiple other factors to consider that could all contribute to your presentation and also delay your rehabilitation and recovery process.
Please consider addressing the following:
Smoking cessation.
Weight loss/management.
Alcohol intake reduction.
Reducing stress levels.
Increase your general exercise.
Improve your sleep.
Addressing all these will assist with the healing recovery process with both non- surgical or surgical management.
Surgery
If your symptoms are severe and have not improved with conservative (non-surgical) management, there are some surgical options. These will depend on the overall condition of the rotator cuff and the shoulder joint.
Subacromial decompression
If there is limited space under the acromion (the roof of the shoulder blade), a subacromial decompression (SAD) may be indicated. The aim of the operation is to increase the space under the acromion. This is an arthroscopic (keyhole) surgery.
Rotator cuff repair
If the tear is acute or the quality of the tissue is good enough, the tendon can be repaired with sutures (stitches).
Reverse shoulder replacement
If you have an extensive rotator cuff tear, osteoarthritis of the shoulder joint and severely restricted function, then a joint replacement may be considered.
Because the rotator cuff is torn, you may need to have a special type of replacement, known as a ‘reverse total shoulder replacement.’ This often helps to reduce your pain, but the amount of movement you have in your shoulder afterwards can be quite limited. Your healthcare professional can give you more advice on this.
Exercises
The following exercise programme has been designed for patients with rotator cuff tears. It will help to build up the strength of the muscles around your shoulder, which should improve their function.
The exercises should be done two to three times a day, for at least 12 weeks. Start the exercises lying down to begin with; as strength increases, move to an inclined sitting position, then to full sitting and finally to a standing position.

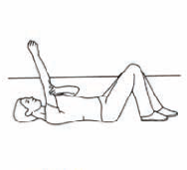
Lying on your back, rest the elbow of your affected arm on a rolled towel.
Bend your elbow as far as possible.
Lift your shoulder to 90 degrees so the elbow points straight up to the ceiling.
Use your other arm to help if needed, but try to make your shoulder muscles work.
Relax and return to the starting position.
Repeat until fatigued, aiming for three minutes
Once your shoulder can reach 90 degrees with your elbow pointing to the ceiling in exercise 1 (arm raises), try to straighten the elbow and point your finger to the ceiling.
Make circular movements with your index finger, then with your wrist and then with your elbow.
Finally, try to make small circles with the whole arm, clockwise and anti-clockwise.
Repeat until fatigued, aiming for three minutes.
To make the exercise harder, increase the size of the circle and/or hold a small weight in your hand (for example, a tin of beans).

Lying on your back, rest the elbow of your affected arm on a rolled towel.
Bend your elbow into the position shown.
Lift your hand straight up into the air and hold for one second before lowering back to the start position.
Repeat until fatigued, aiming for three minutes.
To make the exercise harder, hold a small weight in your hand (for example, a tin of beans).

Once your shoulder can reach 90 degrees with your elbow pointing to the ceiling, following exercise 1 (arm raises), try to straighten your elbow, pointing your finger to the ceiling.
Move your arm up and down in line with your body before returning to the finger-pointing position.
Now, move the arm out to the side and then back across your body.
Repeat each exercise until fatigued, aiming for three minutes.
To make the exercise harder, hold a small weight in your hand (for example, a tin of beans).

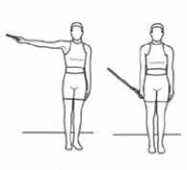
Stand with your elbow bent and hand in a fist position.
Keeping your elbow by your side, rotate your shoulder so your hand moves out, away from your side.
Hold for one second and then move it back into your body.
Repeat until fatigued, aiming for three minutes.
To make the exercise harder, hold a small weight in your hand (for example, a tin of beans).
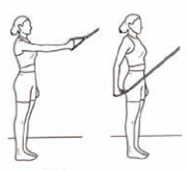
Using an exercise band, tie a know in the band and place the knot over the top of a door.
Close the door to seal the knot on the other side.
With the exercise band hanging down from the top of the door, grasp the end of the band as high up as you can reach with your affected arm.
With a light tension in the band, pull your arm down so your hand is by your side, keeping your elbow straight.
Hold for one second as you check your shoulder posture is square and set well.
Slowly raise your shoulder back up to the start position.
Then, stand side on to the door, perform the same exercise as above, but with your arm going out to the side of you.
Repeat each exercise until fatigued, aiming for three minutes.
Closed-chain exercises

Stand facing a wall with your arms straight and hands on the wall.
Do push-ups against the wall, keeping your body in a straight line.
The further away your feet are from the wall, the more difficult the exercise is to do.
Do not push into an ‘unacceptable pain’ with your exercise.
Repeat until fatigued for three to four sets.
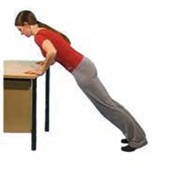
Stand and lean forward onto a table.
Tighten your shoulder blade muscles.
Keep your neck and back straight and slowly do push-ups.
Do not push into an ‘unacceptable pain’ with your exercise.
Repeat until fatigued for three to four sets.
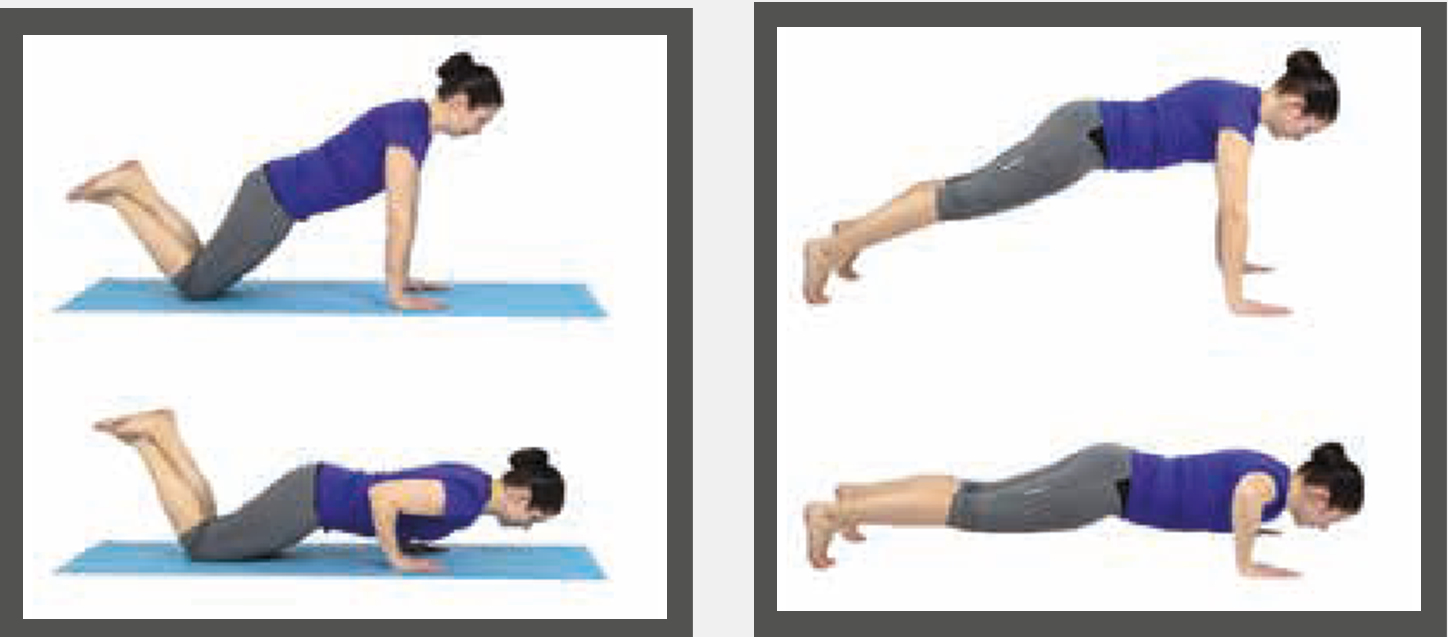
On your hands and knees.
Hands should be shoulder-width apart or narrower.
Keep your body in a straight line.
In a controlled manner, lower your chest close to the floor (keep your elbows close to your body).
Push back up, but make sure you don’t overextend your elbows.
Do not push into an ‘unacceptable pain’ with your exercise.
Repeat until fatigued for three to four sets.

On your toes and hands.
Hands should be slightly wider than level 3.
Keep your buttocks and trunk activated.
In a controlled manner, lower your chest close to the floor.
Push back up, but make sure you don’t overextend your elbows.
Do not push into an ‘unacceptable pain’ with your exercise.
Repeat until fatigued for three to four sets.
Your Health Notts
It is always important to consider other factors that can contribute to musculoskeletal problems and may limit your recovery. The most common factors that can affect your health and wellbeing include smoking, alcohol, weight, stress and general fitness.
There is an excellent resource now available to Nottinghamshire County residents that offers information and guidance on:
- Stopping smoking
- Losing weight
- Alcohol reduction
- Increasing physical activity.
Please visit the Your Health Notts website to find out more or self-refer to this service.
Further sources of information
This document is intended for information purposes only and should not replace advice that your relevant health professional would give you.
External websites may be referred to in specific cases. Any external websites are provided for your information and convenience. We cannot accept responsibility for the information found on them.
Patient Experience Team
The Patient Experience Team (PET) is available to help with any of your compliments, concerns or complaints, and will ensure a prompt and efficient service.
Contact Patient Experience.
Approved
October 2025
Review date
October 2027
Document Id
PIL202510-01-RCT
Service / Department
Musculoskeletal (MSK)
Other formats
Patients who would like this information in an alternative format, or need help communicating with us, please contact our patient experience team.


